20 December 2010
A meta-analysis of eight trials found that patients treated with aspirin were less likely to die from many common cancers during those trials. Follow-up analysis of participants in three of the trials up to 20 years suggested that the benefits persisted, although there did not seem to be beneficial effects on deaths from many cancers during the first five years of treatment. There are significant limitations to the data which mean that a cautious approach to applying these findings is necessary. In particular patients and health professionals must consider the risk of major extracranial bleeds and haemorrhagic stroke with aspirin.
Level of evidence:
Level 1 (good quality patient-oriented evidence) according to the SORT criteria.
Action
These data do not seem to justify routine administration of low dose aspirin to reduce the risk of dying from cancer. Health professionals should be ready to advise those considering this on their risk of cardiovascular events (CV), extracranial bleeds and haemorrhagic stroke – the Cates Plots found below in this Rapid Review may help with this. They should also inform them that the beneficial effects on deaths from many cancers did not appear until aspirin had been taken for five years and were not statistically significant among people who started taking aspirin before the age of 55 years.
What is the background to this?
Several earlier studies have suggested that aspirin may reduce the risk of colorectal cancer. On theoretical grounds, it is possible that aspirin might have a beneficial effect on the risk of certain cancers (adenocarcinomas) at other sites. Observational data suggest that the minimum period required before reductions in cancer risk are observed is about five years.
What does this study claim?
The authors obtained data from eight randomised controlled trials (RCTs) of aspirin for primary or secondary prevention of CV disease which lasted at least four years. Three of the trials also followed up patients with regard to death from cancer for up to 20 years. All analyses were based on intention to treat. The eight trials included 25,570 people, mostly men and the median duration ranged from 4.2 to 8.2 years.
During the period of the trials the pooled odds ratio (OR) for risk of death due to cancer was 0.79 overall (95% confidence interval [CI] 0.68 to 0.92, P=0.003). The risk of death due to cancer was 3.01% in the control group. Applying the pooled OR to this baseline risk suggests a pooled absolute risk reduction of 0.62% (95%CI 0.23% to 0.94%) and a number needed to treat (NNT) of 162 (95%CI 106 to 427) over about 4 to 8 years. However, analysis of patient-level data from seven of the trials (n=23,535) suggests there was no statistically significant reduction in risk in death from any cancer during the first five years of follow up. All-cause mortality was reduced although there was no significant reduction in deaths due to non-cancer causes. The OR for risk of death due to cancer in studies which used 75mg-100mg aspirin daily (n=14,265) was similar to the pooled OR.
Among the three trials where extended follow-up data were available, 10,502 patients took aspirin for at least five years. Over 20 years, there was a reduction in risk of deaths from cancer overall among these patients (NNT=29, 95%CI 19 to 54). However there was no significant effect on haematological cancers and some types of solid cancer. All-cause mortality was reduced at 15 years’ follow up but this effect was not seen at 20 years.
The effect on risk of death from gastrointestinal cancer did not differ by age at randomisation but no effect was seen on the risk of death from any cancer in people who were younger than 55 year at randomisation, and the effect was greater in people aged 65 years or older than in those aged 55 to 64 years at randomisation.
Aspirin seemed to have an effect only on adenocarcinoma, so rates of death from some cancers were not affected. The number of women in the studies was disproportionately low, so it is not possible to know the effects of aspirin on breast and uterine cancer.
So what?
The headline figures of relative reduction in risk of death from cancer of about a fifth over 20 years, or a 1 in 29 chance of benefiting (35 per 1000), seem very attractive. However, clinicians and patients will probably have three questions that need to be considered:
- What are the potential harms of low-dose aspirin?
- How long does aspirin need to be taken for?
- What are my/my patient’s individual absolute chances of benefiting or being harmed?
Firstly, aspirin carries risks, especially of fatal and non-fatal bleeds, including haemorrhagic stroke. No data are presented on fatal and non-fatal bleeds either during the trials or the follow-up period. As discussed in MeReC Rapid Review 359, the ATT meta-analysis of individual patient data from RCTs assessed the benefits on CV events and risks bleeds with long term aspirin, compared with control. The absolute benefits and risks depended on the baseline CV risks of the patients. These are given in graphical format (Cates plots) in the Patient Decision Aid (PDA) for aspirin for primary prevention and below for patients at one level of CV risk below.
The answer to the second question is not clear from this study. In the 20-year follow up analysis, there was no statistically significant reduction in risk of death from cancer among patients whose scheduled in-trial duration of treatment with aspirin was less than five years. There was a greater effect among people scheduled to receive it for 7.5 years or more than those scheduled to receive it for 5 to 7.4 years. However, no data are presented on the consumption of aspirin after the trials finished. This is a potential cause of confounding: perhaps those originally randomised to aspirin stopped taking it, or those randomised to placebo started taking it (e.g. for secondary prevention of CV events). In addition, aspirin treatment was not randomised by baseline history of or risk of cancer.
The final question summarises the previous two. In answering this, much depends on the individual person’s pre-treatment, or baseline, risk of dying from cancer, experiencing a CV event or experiencing a major bleed. The baseline risk of all three increases with age, but not necessarily to the same extent. It is difficult to compare the risks and benefits relating to CV outcomes, major bleeds and cancer death, since available data relate to different time periods and possibly different durations of aspirin treatment. One cannot assume that effects on risk are linear, so we cannot simply multiply a risk per year. In addition, aspirin increases the risk of bleeds and reduces the risk of CV events in the first year of taking it, whereas the beneficial effects on cancer deaths were not seen for about five years (perhaps because of the time required to develop fatal cancer: no data on new diagnoses of non-fatal cancers are reported to allow examination of this idea).
To give some perspective, modelling based on the ATT meta-analysis projected the following benefits and risks of aspirin over 10 years per 1000 people. We have chosen the modelling from the ATT MA for patients with a 20% 10-year CV disease risk, as this seems appropriate to the risk of patients included in the trials in the MA discussed here. This is likely to over-estimate both the absolute increase in risk of bleeds and the reduction in risk of CV events among people at lower baseline CV risk. We have created a Cates plot to illustrate the effect on deaths from cancer during the four to eight years of the trials. This might under-estimate the effects over 10 years, especially if aspirin were taken for 10 years. These Cates plots can be a guide only and must be interpreted cautiously an in the light of the discussion above.
CV events among 1000 people at around 20% 10-year CV risk taking aspirin for 10 years

 Major bleeds among 1000 people at around 20% 10-year CV risk taking aspirin for 10 years
Major bleeds among 1000 people at around 20% 10-year CV risk taking aspirin for 10 years

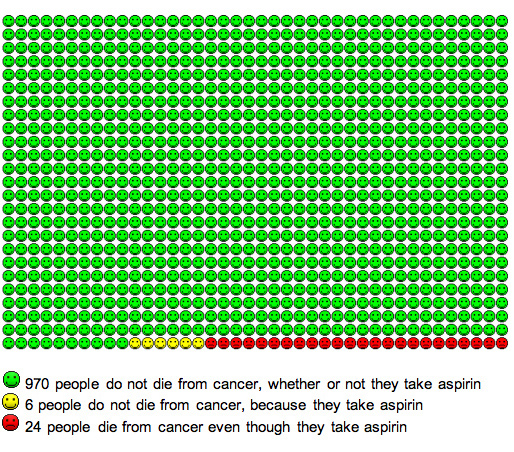
Any death from cancer among 1000 people in this MA taking aspirin for 4.2 to 8.2 years

{kind=link}
{kind=link}
Design Meta-analysis of individual patient data from all eligible RCTs and, where available, long-term follow up individual patient data from cancer registries and death certificates
Patients, intervention and comparison Eight RCTs of 25,570 patients prescribed aspirin vs control for primary or secondary prevention of cardiovascular disease when treatment was scheduled to be for four years or more). Twenty-year follow-up data were available from three UK trials (n=12,659)
Outcomes and results
Deaths during trial period (n=25,570, median duration ranged from 4.2 to 8.2 years)
The pooled OR (fixed effects MA) for risk of death due to cancer was 0.79 overall (95%CI 0.68 to 0.92, P=0.003). The risk of death due to cancer was 3.01% in the control group. This suggests a pooled absolute risk reduction of 0.62% (95%CI 0.23% to 0.94%) and an NNT of about 162 (95%CI 106 to 427) over about 4 to 8 years. The OR was similar in trials of aspirin 75mg–100mg daily (n=14,265) (OR 0.81, 95%CI 0.68 to 0.97, P=0.03).
Where patient-level data were available (seven trials, n=23,535) there was no statistically significant reduction in risk in any cancer during the first five years of follow up. During five or more years’ follow-up, there were reductions in deaths due to cancer but only in either histologically proven adenocarcinomas or primary cancers in which adenocarcinoma predominates.
In-trial all-cause mortality was reduced (10.2% vs 11.1%, OR 0.92, 95%CI 0.85 to 1.00, P=0.047,) although there was no reduction in deaths due to non-cancer causes (OR 0.98, 95%CI 0.89 to 1.07, P=0.63)
Deaths during extended follow -up in patients with scheduled in-trial exposure five years or more (n=10,502, 0–20 years follow -up)
There was a reduction in risk of deaths from cancer overall (HR 0.78, 95%CI 0.70 to 0.87, P<0.0001), including gastrointestinal cancers (HR 0.65, 95%CI 0.53 to 0.78, P<0.0001) and non-gastrointestinal solid cancers (HR 0.79, 95%CI 0.69 to 0.91, P=0.001).
Absolute reductions in risk of death from cancer over 20 years were:
- gastrointestinal cancer 2.18%, 95%CI 1.14 to 3.22, NNT=46, 95%CI 31 to 88
- non-gastrointestinal solid cancer 1.88%, 95%CI 0.57 to 3.19, NNT=53, 95%CI 31 to 175
- any death from cancer 3.49%, 95%CI 1.85 to 5.13, NNT=29, 95%CI 19 to 54.
The effect on risk of death from gastrointestinal cancer did not differ by age at randomisation but no statistically significant effect was seen on the risk of death from any cancer in people who were younger than 55 year at randomisation, and the effect was greater in people aged 65 years or older at randomisation (ARR 7.08%, 95%CI 2.42 to 11.74%) than in those aged 55 to 64 years at randomisation (ARR 4.53% (95%CI 2.06 to 6.99%).
There was no reduction in risk of haematological cancers and the only specific solid cancer subtypes where a statistically significant effect was seen were those of the oesophagus (HR 0.42, 95%CI 0.25 to 0.71, P=0.001), colon/rectum (HR 0.60, 95%CI 0.45 to 0.81, P=0.0007) and lung (HR 0.71, 95%CI 0.58 to 0.89, P=0.002). As was the case for in-trial deaths, where histological data were available the effect of aspirin was confined to adenocarcinomas.
Among the three trials where extended follow-up data were available, 10,502 patients took aspirin for at least five years. Over 20 years, there was a reduction in risk of deaths from cancer overall among these patients (absolute risk reduction 3.49%, 95%CI 1.85 to 5.13, NNT=29, 95%CI 19 to 54). However there was no significant effect on haematological cancers and some types of solid cancer. All-cause mortality was reduced at 15 years’ follow up (HR 0.92, 95%CI 0.86 to 0.99, P=0.03) but this effect was not seen at 20 years (HR 0.96, 95%CI 0.90 to 1.02, P=0.37)
Sponsorship The authors state that this study was completely independent of any pharmaceutical company or other commercial interest.
More information on aspirin can be found on the Antiplatelets section of NPC
Please comment on this blog in the NPC discussion rooms, or using our feedback form.
Make sure you are signed up to NPC Email updates — the free email alerting system that keeps you up to date with the NPC news and outputs relevant to you